Treatment, Article
Green dentistry: agentic AI and the digital path to sustainability
10 April 2026
In the third and final article of a series on “green dentistry”, Christoph Ramseier explores the ways that artificial intelligence can enable periodontists and other dental professionals to act more ecologically in their clinical practice.
The first two articles on green dentistry explored the fundamental principles of sustainable dentistry, showing how reducing single-use plastics, using biodegradable materials, and investing in energy-efficient infrastructure can minimise our ecological footprint. But however much we optimize our materials and equipment, there remains one issue that is often overlooked: the processes themselves and the logistics involved in bringing our patients to our practices. This concluding article looks at how digital artificial intelligence (AI)—specifically agentic AI—can help us to act more ecologically by optimising clinical pathways without compromising clinical excellence.
The next major driver of sustainability in periodontology and dentistry is is the growing integration of digital tools with manual operative procedures. We are entering the age of "agentic AI": autonomous artificial intelligence that not only analyses data but also actively optimises clinical pathways. This technology gives us the opportunity to tackle what the data identify as the biggest source of emissions in our industry: travel. But where exactly do the biggest emissions arise and how can this technology help us address them?
The invisible burden: Logistics and clinical emissions
Duane B, Berners Lee M, White S, Stancliffe R, Steinbach I. (2017). An estimated carbon footprint of NHS primary dental care within England. How can dentistry be more environmentally sustainable? British Dental Journal, 223(8):589-593
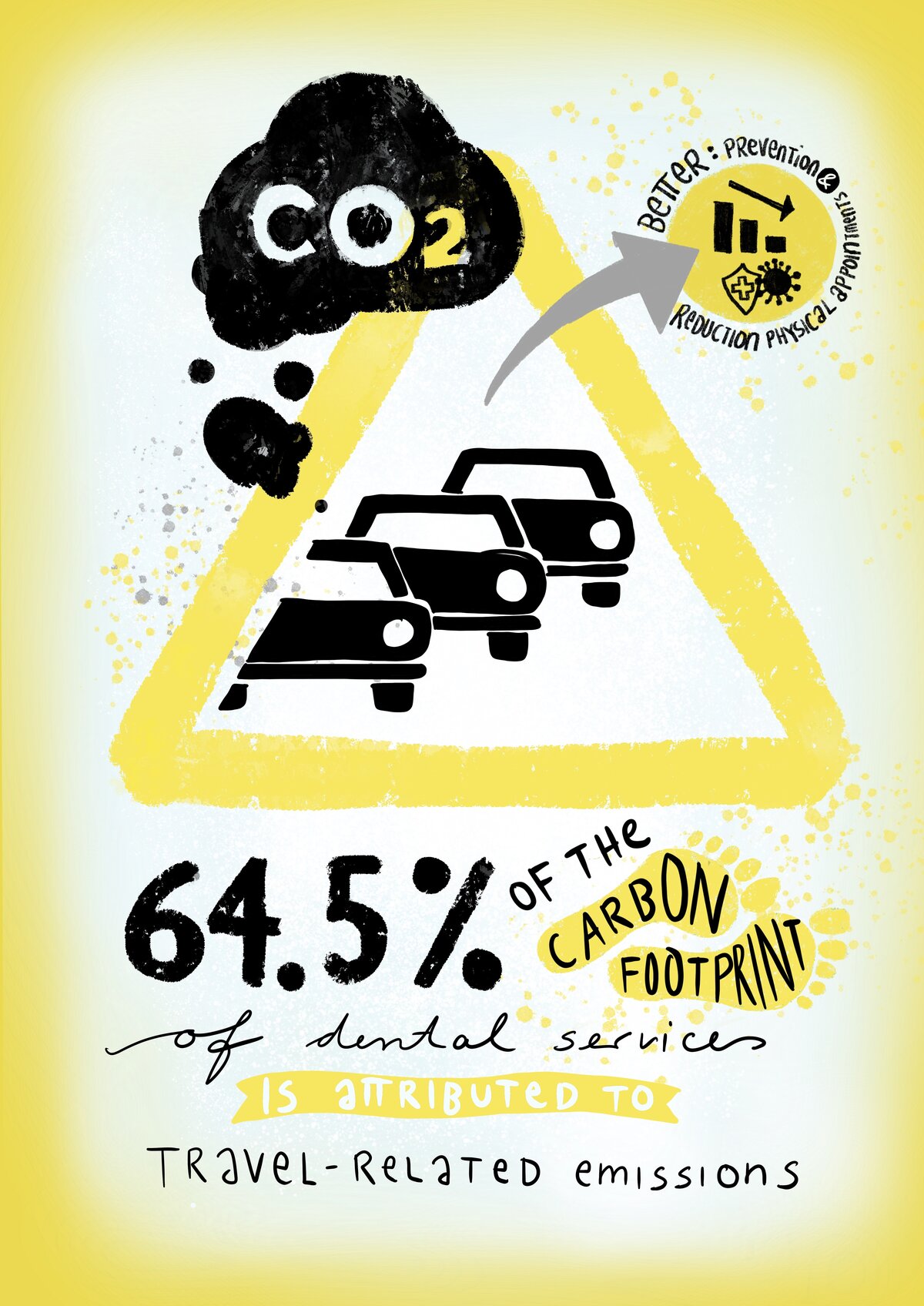
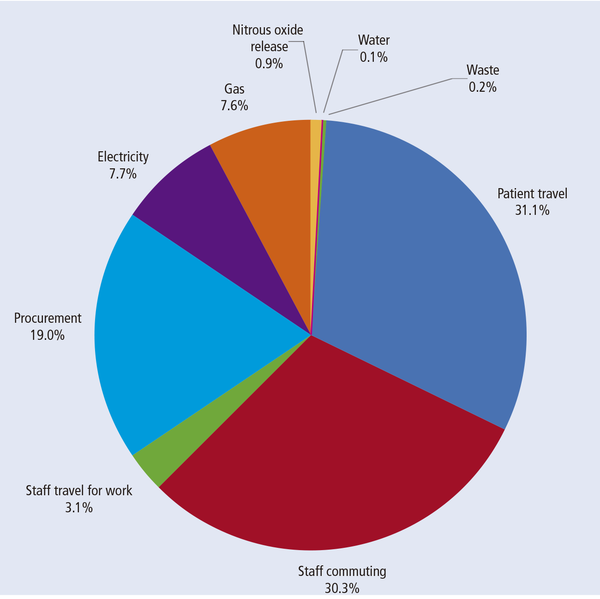
When we think of environmental pollution in dentistry, plastic cups and disposable gloves often spring to mind. However, the data tell a different story. A detailed analysis of the carbon footprint of primary dental services in the National Health Service (NHS) in the UK shows that most of the emissions do not originate in the treatment room, but during the journey to it. In fact, 64.5% of the total carbon footprint of dental services is attributed to travel-related emissions (Duane et al., 2017). Patient travel accounts for 31.1% of this figure, while staff commuting accounts for 30.3%. Other data confirm this, attributing up to 45.6% of emissions to patient travel (Duane et al., 2026). This means that even the greenest dental practice, which separates waste perfectly and sources green energy, has only a limited influence on its overall balance sheet, unless it addresses the traffic volume of its patients. Reducing emissions related to staff is also important and could be achieved by promoting cycling and walking, encouraging the use of public transport, and facilitating remote working through teledentistry and digital tools for consultations and administrative tasks.
Clinical procedures themselves also have an ecological impact. A standard examination generates approximately 5.5kg of CO₂ equivalents (CO₂e), while more complex restorative interventions can generate up to 15kg of CO₂e per session (Duane et al., 2017). A particularly striking example is the use of nitrous oxide, with a single application accounting for up to 119kg of CO₂e, equivalent to the distance driven by an average combustion-engine car for approximately 500 to 600 kilometres. In this study of emissions in NHS dentistry, procurement—all products and services purchased by the clinic, including associated logistics and the supply chain—accounts for 19% of the total carbon footprint (see Figure).
These figures lead to an unavoidable conclusion: the most effective path to greater sustainability lies in avoiding and reducing physical appointments through more precise diagnostics and planning, thereby avoiding complex interventions.
The clinical lever: evidence-based recall intervals
For decades, the six-month recall interval was considered the gold standard for preventing periodontal diseases. However, from ecological and evidence-based perspectives, this dogma must be questioned. Is it sustainable to invite every patient to the practice every six months, regardless of their individual risk?
A comprehensive Cochrane review provides valuable insights on this topic. High-certainty evidence now shows that, for adults, there is little to no difference in clinical outcomes between risk-based and fixed six-month recall intervals over four years. The number of tooth surfaces affected by caries, gingival bleeding, and oral health-related quality of life did not differ significantly between the risk-based and fixed-interval groups. Even when 24-month intervals were compared directly with six-month intervals, there was little to no clinically relevant difference for adults (Fee et al., 2020). This does not mean that we can discontinue care, but rather that we must personalize it. By avoiding unnecessary appointments through precise risk assessment, we can directly reduce the amount of travel-related emissions without endangering our patients' health.
The limitation of human estimation is clear here: to safely extend intervals up to 24 months, we need an exceptionally precise, data-driven risk calculation. This is precisely the area in which artificial intelligence comes into play.
Agentic AI: the future of diagnostics and efficiency
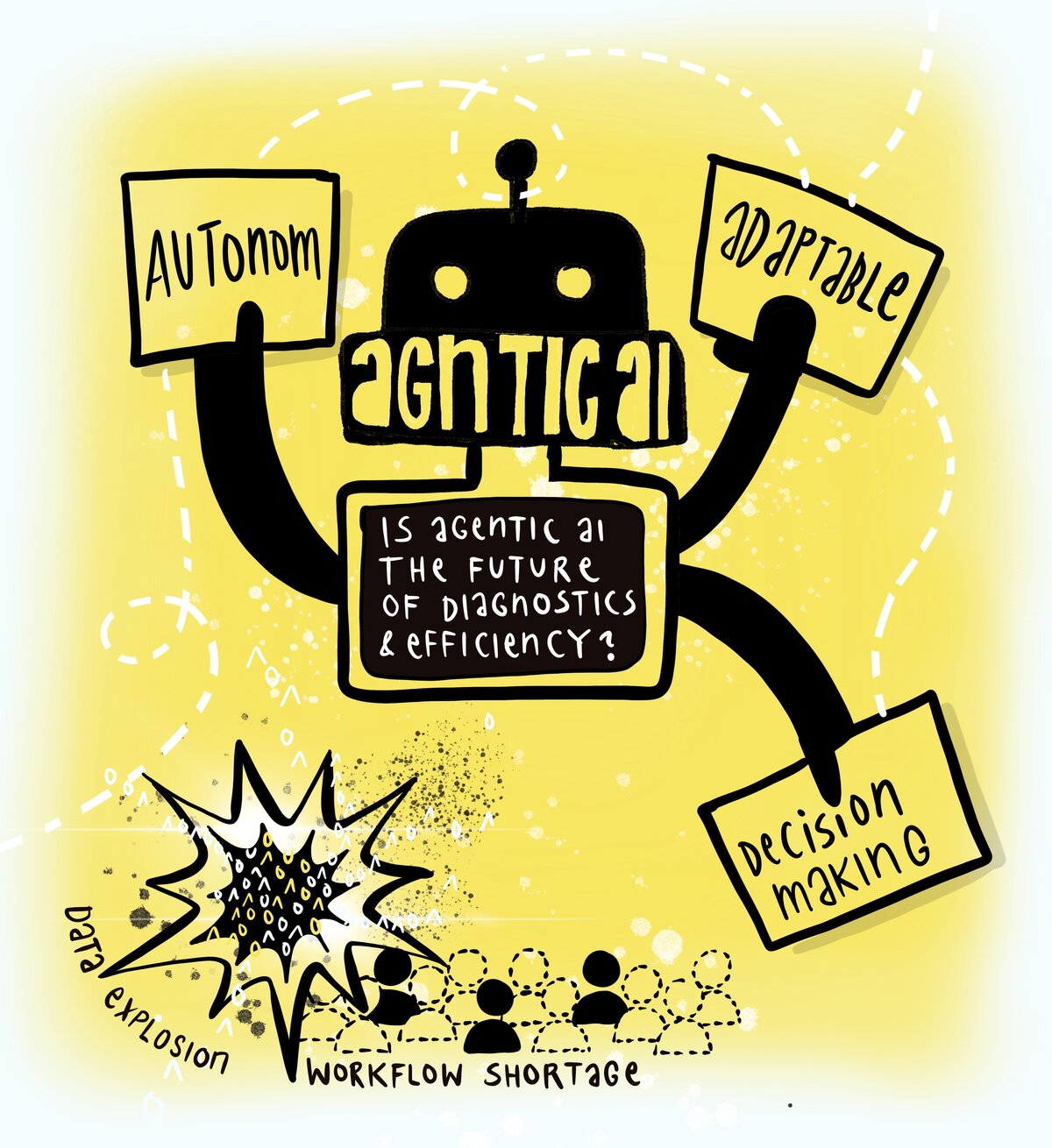
We must distinguish between conventional chatbots and simple algorithms and the new generation of “agentic AI”. While traditional AI systems often react passively to inputs, agentic AI systems are characterized by autonomy, adaptability and probabilistic decision-making. These systems do not simply wait for commands. They act proactively, continuously analyse data streams, autonomously triage patients, and prepare clinical decisions.
The use of such systems is not just a futuristic gadget, but a necessity given two global trends identified in a recent paper on agentic AI in healthcare (Karunanayake, 2025).
- Data explosion: The volume of medical image data grew three- to tenfold between 2011 and 2018. Manual evaluation of this flood of data is becoming increasingly impossible.
- Workforceshortage: A global shortage of 18 million healthcare workers is projected by 2030. Agentic AI is essential to filling this gap and maintaining the quality of care.
In the field of diagnostics, these systems, which were originally developed for use in general medicine and radiology, are already proving superior. Studies on differential diagnosis in MRI scans have shown that AI can achieve an accuracy rate of 61.4%, compared to 46.5% with conventional methods. Specialised AI agents such as “VoxelPrompt” exemplify the potential of agent-based workflows. Rather than merely analysing an image, this tool proactively plans and carries out tasks using external computational tools to segment anatomical structures or characterize pathologies, achieving an accuracy rate of 89%. Similarly, multimodal systems such as “Med-Flamingo”, which are designed to integrate 2D images and text for clinical reasoning, have been shown to improve diagnostic accuracy by up to 20%. These examples from other areas of medicine illustrate the potential for periodontology once the technology is adapted.
In the future, “green dentistry” will mean fewer misdiagnoses and repeat treatments, as well as the precise identification of patients who truly require an in-person appointment.
Green AI: the ecological flip side
Despite all the enthusiasm surrounding digital solutions, we must be realistic: AI is not inherently “green”. The energy consumption of data centres and the training of large models create an ecological footprint of their own. The concept of “sustainable AI” requires us to consider these costs. For example, training a single large deep-learning model can emit around 272 tonnes of CO₂, which is equivalent to the lifetime emissions of five cars (Mehrabanian et al., 2024). Daily usage (“inference”) also adds up: an interactive session with a tool such as ChatGPT (approximately 50 prompts) uses around 50 watt-hours of electricity, equivalent to about 24 grams of CO₂e (Duane et al., 2026). Data centres already consume around 1% of the world's electricity and this figure is rising. The solution lies not in abstinence, but in intelligent usage. Crucial approaches include “green computing”, using smaller, more efficient models, and powering data centres with renewable energy. If we use AI to save thousands of physical patient journeys, the net effect will be positive. Studies suggest that autonomous AI could reduce overall greenhouse gas emissions in healthcare by up to 80% (Ueda et al., 2024).
Practical 'quick wins' and technological synergies
Dental practices can implement practical “quick wins” alongside AI and further optimise them through digital control.
- Teledentistry as an emissions reducer: What began as an emergency solution during the pandemic has become a powerful tool for sustainability. It enables remote consultations and triage, drastically reducing the need for physical visits. Examples from other medical fields demonstrate its potential: in Spain, telemedicine saved over 6,700 tonnes of CO₂ in a single year. In Sweden, telerehabilitation avoided 82,000 km of travel. This is an ideal approach for monitoring progress in periodontology (Di Spirito et al., 2025).
- Intelligent resource management: The hardware in our practices is also becoming smarter. Switching from traditional wet-ring vacuum systems to modern dry vacuum systems can reduce water consumption by up to 85%. Similarly, disposable gloves are an often-overlooked factor, accounting for around 26% of total dental waste. Innovative projects such as the Danish “ReGlove” demonstrate that gloves can be safely reprocessed up to 15 times. The Life Cycle Assessment (LCA) reveals a favourable ecological balance after only the second use (Di Spirito et al., 2025).
Implementation in practice: A roadmap for sustainable innovation
The transformation towards “green dentistry”, supported by agentic AI, is not an abstract concept for the distant future; it is a process that can begin today. For practitioners, this process can be divided into three strategic phases.
Short-term (one to two years): Laying the foundation and harvesting "quick wins". Immediate implementation focuses on reducing obvious waste and introducing basic digital technologies.
- Digital triage: Implement teledentistry for follow-ups and initial consultations to reduce physical appointments and thus travel-related emissions (Di Spirito et al., 2025).
- Evidence-based planning: Move away from rigid six-month recalls for healthy patients. Instead, use existing evidence to extend intervals based on risk up to 24 months (Fee et al., 2020).
- Resource upgrade: switch to dry vacuum systems to reduce water consumption by up to 85% and evaluate the transition to reusable instruments or sustainable disposables (Di Spirito et al., 2025).
- Measurability: Use initial AI-supported tools or carbon calculators to understand your practice's current ecological footprint and identify “hotspots” (Duane et al., 2026).
Medium term (three to five years): Integration of agentic AI and process automation. In this phase, isolated digital solutions are linked into an integrated system.
- Introduce agentic AI: Use advanced AI assistants that autonomously analyse multimodal data (e.g. X-rays and patient records) to offer clinical decision support, thereby increasing diagnostic precision and avoiding mistreatment (Karunanayake, 2025).
- Education: Train your team to use these technologies (“prompt literacy”) and raise awareness of the ecological aspects of digital work (Duane et al., 2026).
- Circular Economy: Look for suppliers offering innovative recycling solutions, such as the reprocessing of gloves, which have a positive ecological balance after just the second use (Di Spirito et al., 2025).
Long-term (six to 10 years and beyond): Systemic resilience and autonomy. The long-term goal is to develop practices that are not only low-emission but also resilient to environmental changes.
- Climatic resilience: Use AI-supported “threshold-based planning” to prepare your practice for unpredictable events (“climatic black swans”) and dynamically manage resources (Gish and Rapaport, 2026).
- Autonomous systems: Rely on fully integrated autonomous AI systems to take over administrative and diagnostic preliminary work, countering workforce shortages and maximising efficiency (Karunanayake, 2025).
- Green computing: When selecting cloud and AI providers, ensure they strictly use renewable energies to maximise the net environmental benefit of AI without creating new ecological debt (Ueda et al., 2024).
Conclusion and outlook: resilience through technology
We live in an era of climate change, which will increasingly expose us to unpredictable extreme weather events, or so-called “climatic black swans”. Our health systems must become more resilient. Agentic AI can help with this by assisting practices and clinics in preparing for such events through “threshold-based planning” and dynamic resource management (Gish and Rapaport, 2026).
The goal is digital, AI-supported dentistry that is more precise and significantly more sustainable. If autonomous AI can deliver even a fraction of the emission reductions projected in early studies (Ueda et al., 2024), the contribution to climate protection will be substantial.
The path to “green dentistry” lies in the intelligent combination of human empathy and machine efficiency. The aim is not to replace dentists, but to give them the freedom to act in a more sustainable, resource-efficient and patient-centred manner through AI. The tools are available—it is now up to the profession to put them into practice.
Bibliography
Di Spirito F, Giordano F, Di Palo MP, De Benedetto G, Aulisio L & Boccia G. (2025). Sustainable Dental and Periodontal Practice: A Narrative Review on the 4R-Framework-Reduce, Reuse, Rethink, Recycle-And Waste Management Rationalization. Dent J (Basel), 13. doi:10.3390/dj13090392.
Duane B, Berners Lee M, White S, Stancliffe R, Steinbach I. (2017). An estimated carbon footprint of NHS primary dental care within England. How can dentistry be more environmentally sustainable? Br Dent J., 223(8):589-593. doi: 10.1038/sj.bdj.2017.839. PMID: 29074898.
Duane B, Ashley P & Larkin J. (2026). Prompt-Driven ChatGPT Carbon Calculator for Dental Practices: Estimation and Tailored Improvement Strategies. International Dental Journal, 76, 103979. doi:10.1016/j.identj.2025.103979.
Fee PA, Riley P, Worthington HV, Clarkson JE, Boyers D & Beirne PV (2020). Recall intervals for oral health in primary care patients. Cochrane Database of Systematic Reviews, 10, CD004346. doi:10.1002/14651858.CD004346.pub5.
Gish M & Rapaport C. (2026). Agentic AI can help hospitals prepare for unprecedented weather. NPJ Digit Med, 9, 73. doi:10.1038/s41746-026-02391-1.
Hsu LP, Huang YK & Chang YC (2022). The implementation of artificial intelligence in dentistry could enhance environmental sustainability. J Dent Sci, 17, 1081-1082. doi:10.1016/j.jds.2022.02.002.
Karunanayake N (2025). Next-generation agentic AI for transforming healthcare. Informatics and Health, 2, 73-83. doi:10.1016/j.infoh.2025.03.001.
Mehrabanian M, Ghorbani F & Alijani S. (2024). Sustainable AI. British Dental Journal, 237, 683. doi:10.1038/s41415-024-8075-3.
Ueda D, Walston SL, Fujita S, Fushimi Y, Tsuboyama T, Kamagata K, Yamada A, Yanagawa M. Ito R, Fujima N, Kawamura M, Nakaura T, Matsui Y, Tatsugami F, Fujioka T, Nozaki T, Hirata K & Naganawa S (2024). Climate change and artificial intelligence in healthcare: Review and recommendations towards a sustainable future. Diagnostic and Interventional Imaging, 105, 453-459. doi:10.1016/j.diii.2024.06.002.
Biography

Christoph A. Ramseier is a Swiss periodontist who received his education and training at the University of Bern. He earned his dental degree in 1995 and his doctorate in dental medicine in 2000. From 1999-2000, he underwent specialised training in periodontology and implantology at the University of Bern, where he became a board-certified specialist in periodontology by the Swiss Society of Periodontology (SSO/SSP) and the European Federation of Periodontology (EFP) in 2004. From 2004-2008, he was a research fellow at the University of Michigan, and in 2024 he became an associate professor in periodontology at the University of Bern, where his research focuses on periodontal risk management and supportive periodontal care.
EFP partners


Sign up to our newsletter
The EFP publishes a free monthtly email newsletter with the latest news about the federation's activities, its publications, and its campaigns.