
Issue No. 149
Summarized from Journal of Clinical Periodontology, Volume 53, Issue 5, May 2026, 658-680
Editor: James Deschner, chair, EFP scientific affairs committee
What are the treatment outcomes of different surgical protocols for peri-implantitis?
Authors: Wenjie Zhou, Ausra Ramanauskaite, Clemens Raabe, Emilio A Cafferata, Neelam Lingwal, Frank Schwarz
Background
Peri-implantitis is a condition with a high prevalence and is considered a significant clinical challenge in implant dentistry. Effective therapeutic strategies to prevent disease progression and preserve implant function are needed.
Non-surgical interventions have demonstrated limited and inconsistent efficacy. Therefore, surgical and combined treatment approaches are indicated.
The primary objective of surgical therapy is to re-establish peri-implant tissue health and ensure the long-term stability of both soft and hard tissues. Reconstructive surgical procedures additionally aim to regenerate peri-implant bone defects, promote re-osseointegration, and maintain stable tissue conditions postoperatively.
Despite the availability of diverse surgical techniques, treatment outcomes remain difficult to predict and recurring inflammation and progressive bone loss are commonly reported. Such complications may necessitate further surgical intervention or implant removal.
Aim
To assess the treatment outcomes of surgical peri-implantitis treatments performed by trained surgeons by analysing the results from between six months and five years after treatment, and to identify the factors that influence treatment success.
Materials and methods
- Retrospective cohort analysis performed by two investigators at the Department of Oral Surgery and Implantology of Goethe University in Frankfurt, Germany.
- Inclusion criteria: presence of at least one screw-type implant with peri-implantitis, which was surgically treated in patients diagnosed and treated for chronic periodontitis.
- Exclusion criteria: uncontrolled systemic disorders affecting bone metabolism, zirconia/machine surfaced implants.
- The outcomes of four different treatment procedures were assessed at different timepoints (baseline, six months, one year, two years, three years, four years and five years):
- Open-flap debridement (OFD)
- Implantoplasty
- Reconstructive therapy (REC)
- Combined treatment (implantoplasty + REC).
- Clinical outcome measures—plaque, bleeding on probing (BOP), suppuration, mean probing depth (PD), maximum PD, soft-tissue recession, mean width of keratinized mucosa—were recorded at six sites per implant, except for keratinized mucosa, which was measured only at the three buccal sites.
- The primary outcome was treatment success after one year, defined according to three different combination criteria:
- maximum PD £5 mm, £1 BOP site and no suppuration.
- reduction in mean PD, £2 BOP sites and no suppuration.
- reduction in maximum PD, £2 BOP sites and no suppuration.
- Secondary outcomes were mean values in the clinical parameters at baseline and follow-up visits, implant loss,and the need for surgical retreatment.
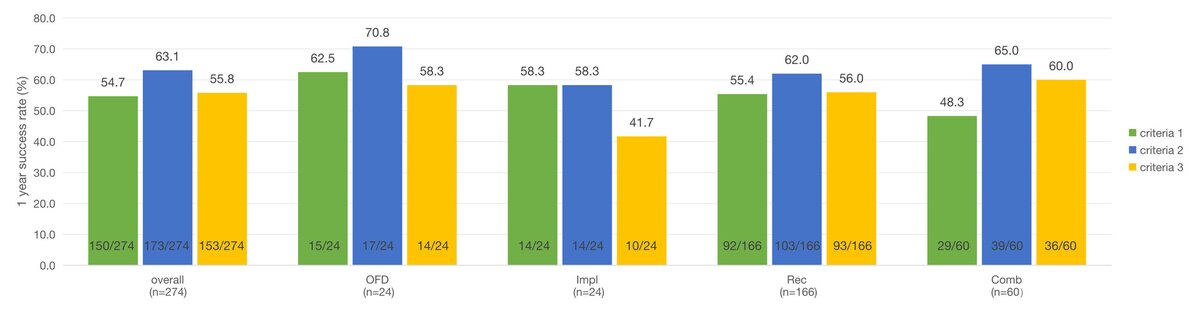
Bars represent the percentage of successful implants according to criteria 1–3 at T2. Numbers on top of bars indicate success rates (%). Fractions at the bottom inside each bar indicate the number of successful implants relative to the total implants in each group (x/n).
Results
- A total of 223 patients with 406 implants were included in the analysis, treated using four surgical modalities (OFD, implantoplasty, reconstructive therapy, and combined approaches).
- Treatment success at one year was 54.7%, with no statistically significant differences between the different surgical techniques.
- Across the various follow-up time points, success rates decreased over time, dropping to 27–30% after five years, indicating limited long-term stability.
- Over a mean follow-up period of approximately 31 months, 9.9% of implants were lost and 37% required retreatment. Non-surgical retreatment was performed on 133 (32.8%) implants in 85 patients, and surgical retreatment was performed on 38 (9.4%) implants in 22 patients.
- Although the combined treatment group showed higher rates of implant loss and retreatment, these differences were only statistically significant for the retreatment.
- All treatment modalities resulted in comparable improvements in clinical parameters (e.g., probing depth, bleeding on probing, suppuration), with no significant differences between groups.
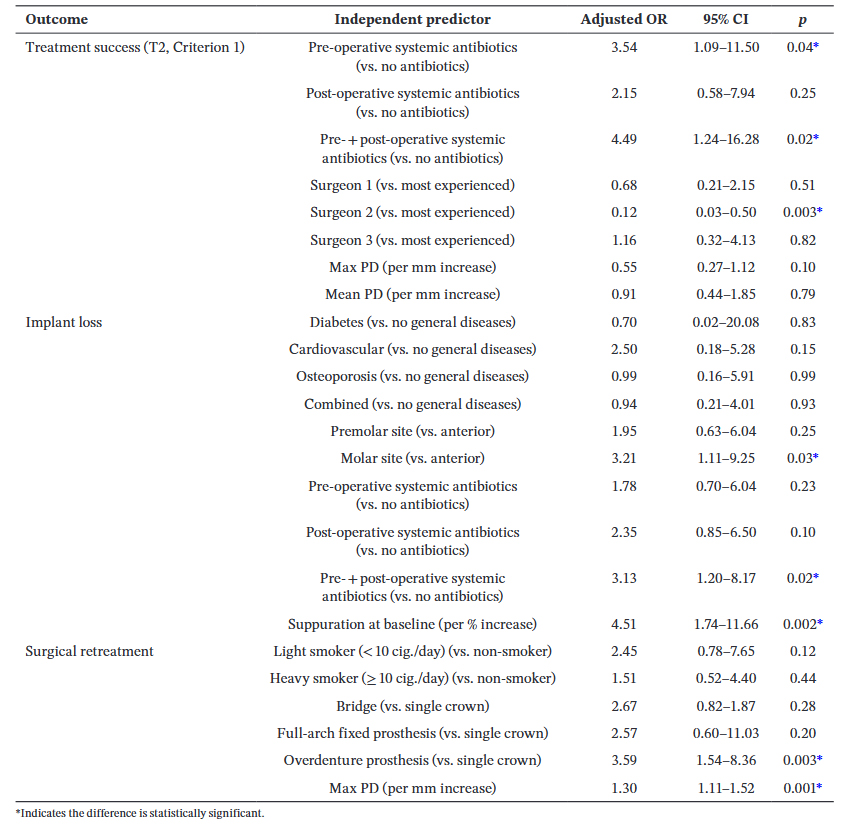
- Regression analyses identified several factors associated with treatment outcomes:
- Treatment success was positively associated with the use of systemic antibiotics (only in short-term results: one year) and surgeon-related factors (operator variability.)
- Implant loss was associated with molar implant location, baseline suppuration, and the use of antibiotics both pre- and post-operatively during the longer follow-up period.
- The need for surgical retreatment was associated with overdenture prostheses and greater baseline maximum PD.
- Overall, the findings indicate that clinical outcomes are influenced more by patient-, implant-, and operator-related factors than by the specific surgical technique applied.
Limitations
- Single-centre university-based study.
- Limited sample size with group imbalance.
- Heterogeneity in defect morphology and lack of information about defect configuration.
- Retrospective design and therefore non-randomized treatment protocols.
- Surgeon-related differences and detection bias by the treating surgeon.
- Not always a fixed follow-up.
- Lack of standardized radiographic follow-up.
- Antibiotic use (not based on predefined criteria).
Conclusions and impact
- This study found that the success rate of the surgical treatment for peri-implantitis, regardless of the treatment modality, was 54.7% after one year.
- Treatment outcomes were positively linked to surgeon-related factors.
- While short-term outcomes were positively linked to the use of systemic antibiotics, for long-term outcomes their use was linked to implant loss.
- Implant loss was more likely to appear at molar sites and in the presence of baseline suppuration.
- The need for surgical retreatment was associated with overdentures and a deeper baseline PD.
Treatment success depends on multiple factors, including patient case selection and the surgeon, but not on different surgical techniques.
Rapporteurs: Jantine Florine Yntema, Celestine Franca Overtoom, and Kyriaki Diamantopoulou, supervised by Monique M. Danser
Affiliation: Postgraduate programme in periodontology, ACTA. Amsterdam, Netherlands
With kind permission from Wiley Online Library. Copyright © 1999-2026 John Wiley & Sons, Inc. All rights reserved
EFP partners


Sign up to our newsletter
The EFP publishes a free monthly email newsletter with the latest news about the federation's activities, its publications, and its campaigns.