Clinical & Translational Research, Article
Soft-tissue augmentation around dental implants: CTG or CMX?
15 June 2026
What is the best approach for augmenting peri-implant soft-tissues? Lenz Surdiacourt (Ghent University, Belgium) winner of the first prize for clinical research in the latest edition of the EFP’s annual Postgraduate Research Prize, describes a randomized controlled trail comparing the “gold standard” connective-tissue graft and the alternative approach of collagen matrix.
Thick peri-implant mucosa is associated with improved aesthetic outcomes and increased soft-tissue stability. Although connective-tissue grafting (CTG) remains the gold standard for augmenting peri-implant soft tissues, it requires a second (donor) surgical site, which increases patient discomfort.
As a result, xenogeneic collagen matrices—including cross-linked porcine-derived matrices, designed to preserve volumetric stability—have been developed as alternatives. Because long-term clinical data on these matrices are limited, we initiated a multicentre, randomized controlled trial to compare CTG with a porcine-derived collagen matrix (CMX) for soft-tissue augmentation at single-tooth gaps.
Sixty patients with a single-tooth gap in the premaxilla and a minor horizontal mucosal defect were randomized to CTG (control) or CMX (test). All patients underwent immediate restoration of single implants using a standardized digital workflow. Following implant placement, CTG or CMX was trimmed to the site-specific dimensions and inserted into the buccal envelope (Figure 1). Follow-up assessments were performed immediately postoperative (T1) and at three months (T2), one year (T3), and three years (T4); a five-year follow-up is planned.
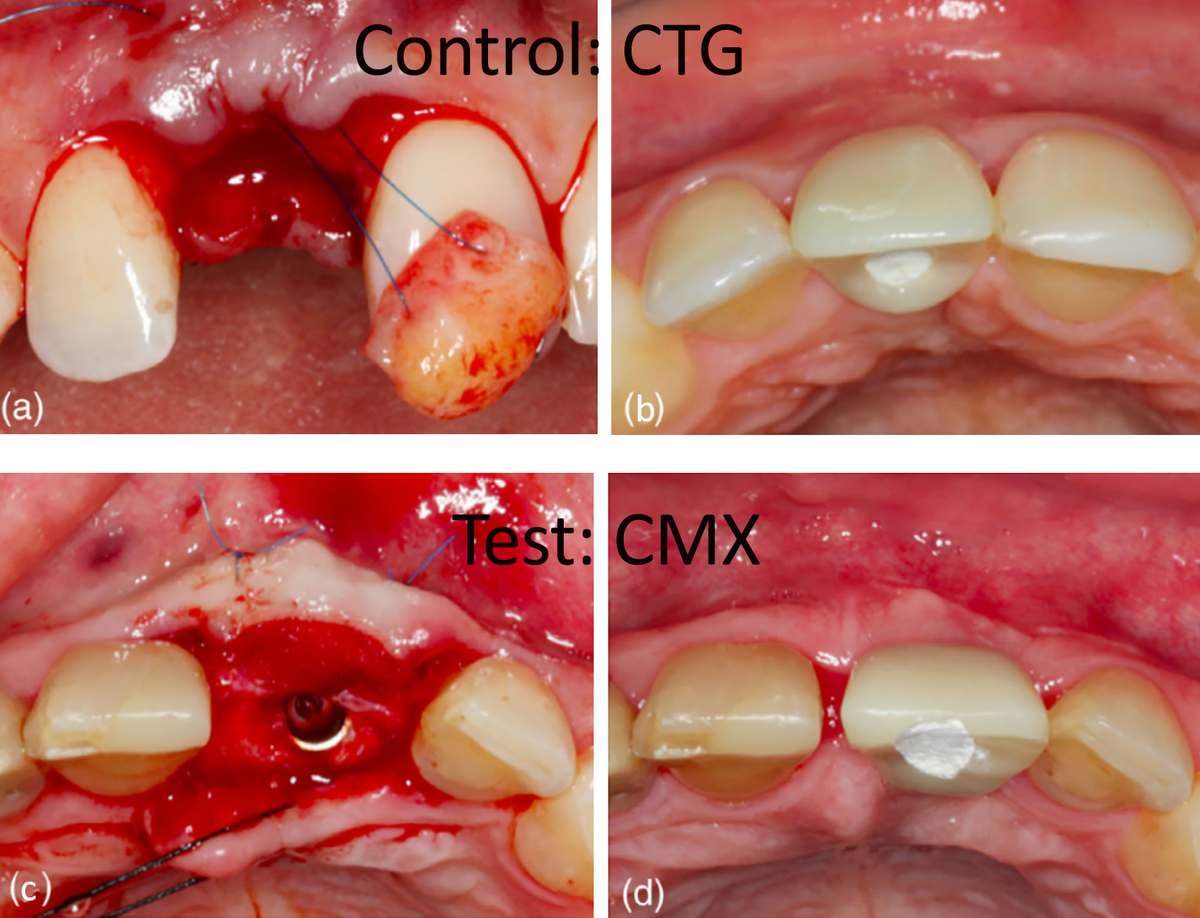
BOTTOM: Case illustrating a patient of the test group (CMX): (c) occlusal view of CMX brought into the buccal envelope and fixed with two single sutures; (d) occlusal view at three months follow-up.
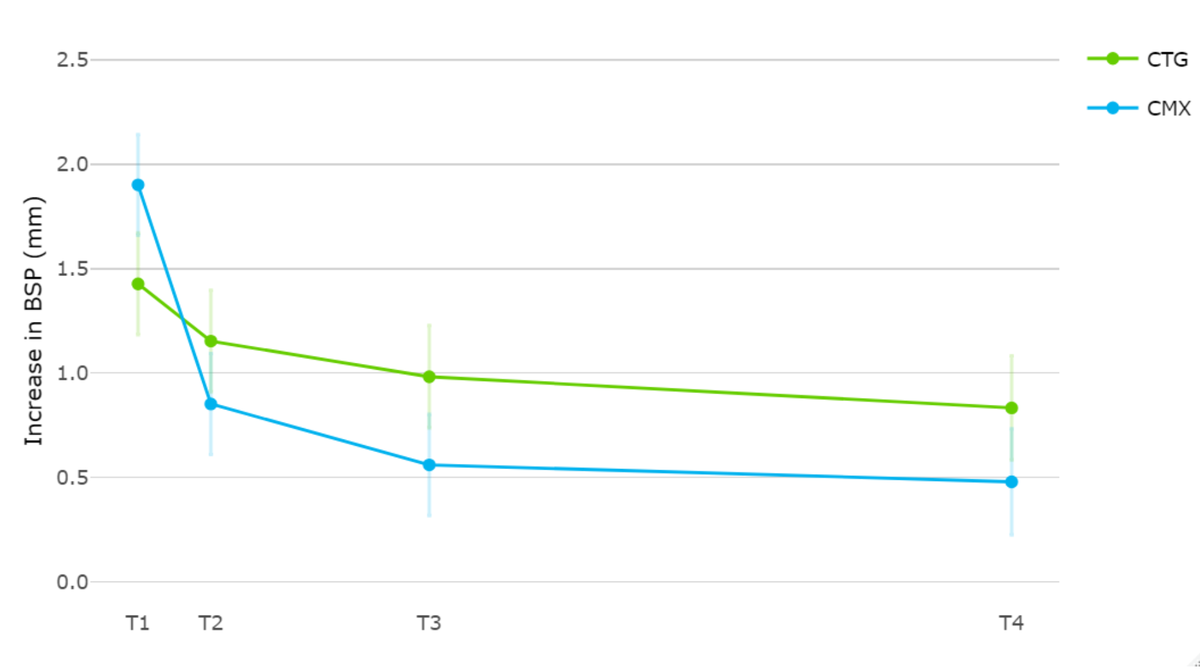
The primary outcome was the increase in the buccal soft-tissue profile (BSP), which was analysed using superimposed intraoral scans. Secondary outcomes included soft-tissue healing dynamics and marginal bone loss (MBL), as measured on periapical radiographs.
Different soft-tissue healing dynamics were seen between groups. Immediately postoperatively (T1), the CMX group demonstrated a statistically significant advantage in BSP compared with CTG. However, after three months (T2), the effect reversed in favour of the CTG group, and this relative difference persisted to the three-year follow-up (T4) (Figure 2).
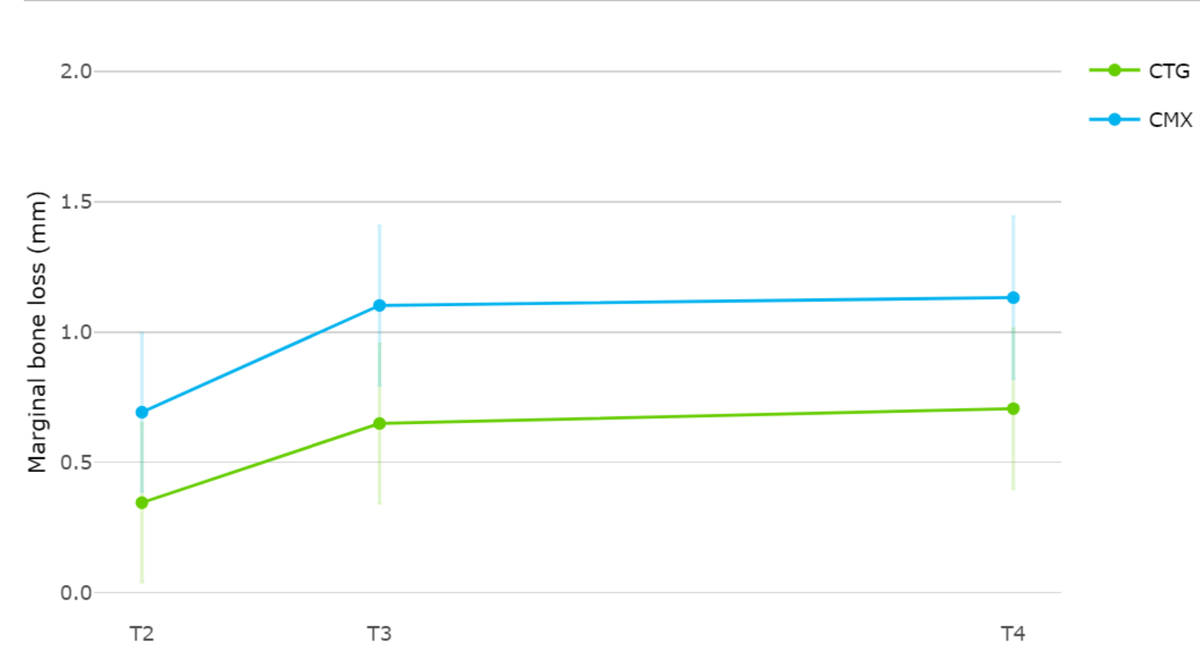
The CMX group exhibited greater marginal bone loss during the early healing phase as compared to the control group. This difference between the two groups was maintained during the follow-up (Figure 3).
Within the limits of the present study, CTG remains the gold standard for soft-tissue augmentation in terms of increasing the buccal soft-tissue thickness. CMX may offer clinical indications to simplify surgery and avoid donor-site morbidity. Clinicians should be aware of its greater early resorption and the associated increase in marginal bone loss observed in this study.
Longer-term follow-up is needed to assess the long-term stability of the mucosal thickness and the marginal bone loss.
Biography

Lenz Surdiacourt earned his dental degree from Ghent University, where he subsequently completed specialist training in periodontology and oral implantology. During his postgraduate programme he initiated a PhD project investigating the use of soft-tissue substitutes around dental implants. He currently combines his research with clinical work in private practices.
EFP partners


Sign up to our newsletter
The EFP publishes a free monthly email newsletter with the latest news about the federation's activities, its publications, and its campaigns.