Perio Workshop 2012
VIII European Workshop on Periodontology
Periodontitis and systemic diseases
11-14 November 2012
The 8th European Workshop in Periodontology: “Periodontitis and systemic diseases” took place from November 11 to 14, 2012 and involved over 90 of the world’s leading dental experts in an intense scientific review process of evidence linking oral diseases to general illnesses in three study areas: diabetes, cardiovascular disease, and pregnancy.
This event was major in more ways than one: it was the first specific gathering to bring together members of both the European Federation of Periodontology and the American Academy of Periodontology, and was jointly organised by these two prestigious dental organisations. But beyond conquering logistical difficulties (and even a general strike by Spanish workers on the last day of the Workshop), the matters under such careful scrutiny by the Workshop’s three working groups have great transcendence for the medical community as a whole and for public health.
Held in the sumptuous historic surroundings of La Granja de San Ildefonso, a tiny Spanish town outside Segovia which lives up to its grand-sounding name and boasts a Royal Palace set amongst chocolate box street views, the three working groups – DIABETES; CARDIOVASCULAR DISEASE; ADVERSE PREGNANCY OUTCOMES – gathered early each morning to pore over the many papers and studies which have confirmed associations between periodontitis and the systemic illnesses.
As part of a careful process involving long and taxing sessions of debate and analysis, these scientists worked towards the creation of consensus reports on each subtopic. Their work sought to establish to sort and clarify evidence in the key areas of the interrelation between oral and general health: epidemiological association, risk factors, pathogenic mechanisms, and greater health implications.
These conclusions were published in 2013 in special editions of the Journal of Clinical Periodontology (EFP) and the Journal of Periodontology (AAP).
The importance of the themes under scrutiny at this Workshop has given rise to a comprehensive and carefully monitored communication strategy to create widespread awareness of its aims and conclusions.
A documentary video was filmed during the three days in La Granja, and was given an international presentation on March 15 at the EFP General Assembly in Jerusalem. It features interviews with experts and chairmen of the Workshop working groups as they explain the extent of current research, the way to move forward in future investigation, and what recommendations the periodontal community has for dentistry and the medical community as a whole.
An ongoing media campaign was co-ordinated and executed by the EFP’s own communications team and a top European press agency with years of experience in the medical field.
EFP
| Mariano Sanz | Facultad de Odontología Universidad Complutense de Madrid P. Ramón y Cajal s/n 28040 Madrid Madrid Spain |
| Iain Chapple | Periodontal Research Group College of Medical and Dental Sciences The University of Birmingham St. Chad’s Queensway Birmingham B4 6NN, UK |
| Maurizio Tonetti | Executive Director, European Research Group on Periodontology, Italy Via Don Minetti, 10 16126 Genova, Italy |
AAP
| Robert Genco | Department of Oral Biology, State University of New York at Buffalo, Baird Research Park, 1576 Sweet Home Road, Amherst, NY 14228, USA. |
| Thomas E. Van Dyke | Department of Periodontology The Forsyth Institute Cambridge MA 02142, USA |
| Kenneth Kornman | Interleukin Genetics Waltham, Massachusetts, USA |
Working groups
Group 1: Cardiovascular Disease and Periodontal Disease
| Chair | Thomas E. Van Dyke, Maurizio Tonetti |
| Reviewer | Frank Scannapieco, Jim Beck, Ann Progulske-Fox, Arien Van Winkelhoff, Harvey Schenkein, John Gunsolley, Thomas Dietrich, David Herrera, Bruno Loos, Francesco D’Aiuto |
| EFP | Philippe Bouchard, Søren Jensen, Stefan Renvert, Filippo Graziani, Palle Holmstrup |
| Guest | Mark Bartold, Michael Glick |
| AAP | Ray Williams , Paul Eke, Tom Hart, Angelo Mariotti, Chris Cutler, Alpdogan Kantarci, Mark Herzberg |
Group 2: Diabetes and Periodontal Disease
| Chair | Iain Chapple, Robert Genco |
| Reviewer | Wenche Borgnakke, George Taylor, Pekka Yiostalo, John Taylor, Philip Preshaw, Evanthia Lalla, Steve Engebretson, Thomas Kocher |
| EFP | Tord Berglundh, Ubele van der Velden, Joerg Meyle, Klaus Lang, Eickholz Peter, Clemens Walter, Wilem Nesse, Francis Hughes |
| AAP | Ira Lamster, Dana Graves, Sara Grossi, Hatice Hasturk, Brian Mealey, David Paquette, Wenche Borgnakke |
| Colgate | Veronique Moy |
Group 3: Adverse Pregnancy Outcomes (APOs) and Periodontal Disease
| Chair | Mariano Sanz, Kenneth Kornman |
| Reviewer | Gerard Linden, Mark Ide, Anders Gustafsson, Phoebus Madianos, Panos Papapanou, Steve Offenbacher, Bryan Michalowicz |
| EFP | Lior Shapira, LeoTrombelli, Gernot Wimmer, Björn Klinge, Tellervo Tervonen, Marc Quirynen |
| AAP | Michael Reddy, Ricardo Teles, James Katancik, Michael Rethman, Yiping Han, Laurie McCauley |
| Colgate | Manuel Voegtli, Barbara Shearer |

Perio and cardio – the links and what they mean for dental practice
Atherosclerotic cardiovascular diseases (ACVDs) are a leading cause of death and disability across the developed world and impose a vast burden on healthcare resources. This category of diseases includes:
- Coronary heart disease, which presents as angina or heart attack (myocardial infarction).
- Ischaemic cerebrovascular disease, which may manifest as stroke or mini-stroke (transient ischaemic attack or TIA).
- Peripheral vascular disease.
Periodontitis, although not a cause of mortality, is also a major public health concern because of its high prevalence in the population and its negative impact on oral health, ability to chew, appearance, quality of life, dental care costs and tooth loss. In addition, as a progressive, chronic inflammatory disease, untreated periodontitis has the potential to undermine overall health and even exacerbate other inflammatory conditions, such as ACVD.
Recently, an international panel of leading clinicians and research scientists convened at a landmark meeting in Spain, organised jointly by the European Federation of Periodontology (EFP) and the American Academy of Periodontology (AAP), to review the latest scientific research into periodontitis and ACVD. The EFP is one of the foremost dental organisations in Europe, with a membership comprising 26 National Periodontal Societies with over 13,000 members, and works to promote awareness and understanding of, and best practice within periodontology. The AAP is the leading professional organisation for periodontists in the United States, with a membership of more than 8,000 specialists.
After a detailed systematic review of the evidence, the experts produced a consensus report outlining our current understanding of the relationship between periodontitis and atherosclerotic cardiovascular disease. They also formulated new evidence-based guidelines for general dental practice. A brief summary of their findings is presented here, followed by the new professional recommendations.
Effects of periodontitis on the incidence of cardiovascular events
Periodontitis has been shown to increase the risk of a first ACVD event, (such as heart attack or stroke), independent of other known cardiovascular risk factors. The size of the increase in risk varies according to the type of ACVD event, and also depends upon age and gender. For example, the extra risk posed by periodontitis is greater for cerebrovascular disease than for coronary heart disease, and also greater in males and in younger people (studies show no increased risk in individuals aged 65 years or more). However, given the high prevalence of periodontitis in the population, it is clear that even a low-to-moderate increase in risk has important implications for public health.
Although some risk factors, such as smoking and diabetes, are known to play a role in the development of both periodontitis and ACVD, their presence does not fully explain the observed link between periodontitis and the increased cardiovascular risk. Moreover, additional risk due to periodontitis was shown in people who had never smoked and was also apparent in studies that controlled for diabetes status. It is possible, however, that there are as yet unknown genetic factors that may influence both of these inflammatory diseases and may therefore explain the association found in clinical studies.
At the moment, there is not enough evidence to show whether periodontitis could increase the probability of a second ACVD event in patients with established ACVD who have previously suffered an event.
What is the link between periodontitis and ACVD?
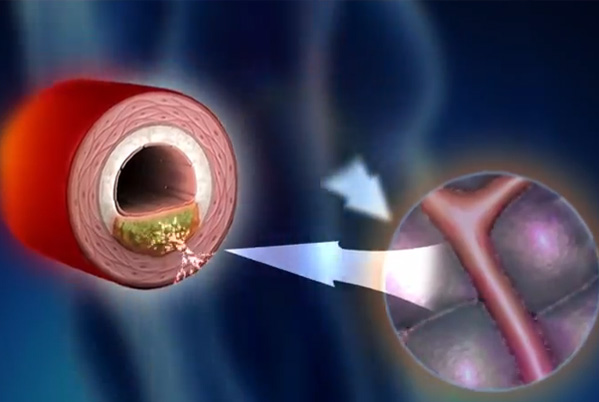
The most likely explanation for how periodontitis affects ACVD is that periodontal bacteria and their products (e.g. endotoxin) from periodontal pockets enter the circulation and provoke an acute-phase and subsequent inflammatory response. Mediators produced as part of this host response then promote the development, maturation and instability of fatty lesions (atheroma) in the arteries, increasing the risk of an ACVD adverse event.
Research shows that the likelihood of periodontal bacteria entering the bloodstream (bacteraemia) after chewing, brushing, flossing or scaling depends upon the patient’s periodontal health. Bacteraemia is more common, and involves a wider range of bacteria (including periodontal pathogens), in patients with periodontitis, compared with patients who have gingivitis or healthy mouths.
Further support for the direct involvement of periodontal bacteria in ACVD has come from studies demonstrating:
- a link between the prevalence of bacteraemia and plaque/gingival indices
- the presence of periodontal pathogens in atherothrombotic lesions, and a correlation with periodontal status
- a correlation between the subgingival flora and pathogens detected in atheroma
- live and viable periodontal bacteria living within atheroma.
Another possible mechanism by which periodontitis might contribute to ACVD risk is that antibodies produced in response to plaque bacteria may promote the development of atheroma by cross- reacting with the cells lining the arteries (endothelial cells) and with blood lipids.
What are the effects of periodontal treatment on cardiovascular outcomes?
Studies have demonstrated that periodontal treatment reduces the overall level of inflammation within the circulation. Specifically, periodontal therapy had favourable effects on two key factors known to be important in ACVD risk: levels of a pro-inflammatory acute-phase protein agent called C-reactive protein (CRP); and measures of endothelial cell function. Cholesterol levels, however, were not affected by treatment.
More limited evidence suggests that periodontal therapy improves other known markers of inflammation, coagulation and endothelial cell activation, and also arterial blood pressure and subclinical ACVD.
To date, no intervention studies have tested the effect of periodontal treatment on preventing first ACVD events (primary prevention) or on preventing recurrence (secondary prevention). The focus has been on surrogate endpoints such as vascular stiffness and biomarkers of cardiovascular risk. Further research is needed, in carefully selected patient populations (< 65 years of age, preferably) with well-defined minimum disease levels and treatment goals, to explore the possible benefits of periodontal treatment on cardiovascular health.
Can ACVD treatments influence treatment outcomes for periodontitis?
There is some new evidence that various anti-inflammatory agents prescribed to patients with ACVD – such as aspirin, statins, fish oil and vitamin D – may also help reduce periodontal inflammation.
Implications for general dental practice
There is gathering evidence that periodontitis is a risk factor for future cardiovascular disease and that periodontal therapy can reduce systemic inflammation. It follows that effective prevention and early treatment of periodontitis may have an important role in reducing an individual’s susceptibility to ACVD events and also in contributing to improved cardiovascular health at a population level. Patients should therefore be advised about the health risk associated with untreated periodontitis, particularly if they have other ACVD risk factors, and offered comprehensive periodontal care and advice. In patients who have suffered an ACVD event, good oral hygiene should be established and periodontal treatment staggered over several sessions, in order to minimize the magnitude of any intra-operative bacteraemia and the subsequent inflammatory sequelae.
Perio and diabetes
Diabetes and gum disease
Diabetes is a very common health problem that, if not well controlled, can have many serious health effects. In type 2 diabetes – by far the most common form – sugar (glucose) levels in the bloodstream are higher than normal. This may be because the body is not making enough of the hormone insulin, which is needed to help cells take up sugar from the blood to use for energy or energy storage, or because the body is not responding to its insulin as well as it should, or for both of these reasons. This type of diabetes usually starts in middle age and is often linked to being overweight and having a sedentary lifestyle, but it is becoming very common in younger people, even in children. The diabetes problem affects all populations and is becoming a “global epidemic” whose complications include sufferers being more likely to develop conditions such as heart and kidney disease, leading in turn to a lower life expectancy.
Gum disease is one of the most common diseases seen in humans. In its most severe form, known as periodontitis, the gum tissue and bone that support the teeth are destroyed over time, leading to loss of teeth. Periodontitis affects about half of all adults and as many as 85% of people over 65-years of age.
Although diabetes and gum disease may seem like very different diseases, dentists have known for a long time that people with diabetes are more likely to get gum disease. Also, their gum disease may be worse and harder to treat, compared with people who do not have diabetes. If a person’s blood sugar levels are under good control, however, gum treatment is more likely to be successful. But that’s not the end of the story: scientists are now finding that gum disease may also have an effect on diabetes, making blood sugar control more difficult. Is is clear and that keeping the gums healthy is an important part of looking after the overall health of a person with diabetes.
How gum disease can affect diabetes
At a recent meeting of top experts in dental and diabetes research from around the world, scientists looked closely at all the latest research into diabetes and gum disease to reach an agreement on, and to find a new understanding of how these two diseases might affect one another. They found that:
- In people with diabetes, those who have severe gum disease have higher blood sugar levels (measured by a test called HbA1c), compared with those with healthier gums
- Even in you don’t have diabetes, your body’s control of blood sugar levels is not as good as it should be when you have severe gum disease
- The worse the gum disease, the more likely a person is to go on to suffer damage to other organs in their body because of their diabetes – for example, heart or kidney disease
- Having severe gum disease might actually increase your chance of getting type 2 diabetes.
Why does gum disease affect diabetes?
It is not yet completely understood why gum disease should have an effect on diabetes, but scientists think that some of the germs that infect the gums when we get gum disease can escape into the bloodstream. This triggers a reaction from our body’s defence system, which can lead to the release of powerful molecules that have harmful effects on other parts of the body, resulting in worsened blood sugar control.
Can gum treatment help diabetes control?
The good news is that treatment for gum disease, such as the professional cleaning and regular care given by your dentist or hygienist, can lead to a fall in blood sugar levels in some people with diabetes. The improvement is about the same as you might have if you added a second drug to your usual diabetes medication. This means that, if you have diabetes, improving your gum health could really help you control your diabetes and may also help lower your risk of diabetes complications. If you don’t have diabetes but think you have a chance of getting it (maybe because it’s in your family), having any gum disease treated is one of the things that might help you to stay healthy, alongside losing weight and taking exercise, as advised by your doctor.
The latest research on gum disease and diabetes shows the importance of keeping your gums as healthy as possible by careful cleaning at home and having regular dental check-ups. That way, any gum disease can be picked up early and treated. Having healthy gums is an important step towards better overall health.

Perio & Pregnancy

Pregnancy and gum disease
For most women, pregnancy is a natural part of life that leads to the birth of a healthy baby. Sometimes, however, women may have some problems during their pregnancy. These may cause their baby to have a low weight at birth, or to be born earlier than usual, or not to grow properly in the womb. Some pregnant women suffer from a serious problem called pre-eclampsia (very high blood pressure is one sign of this). Others sadly lose their baby because of a miscarriage or stillbirth.
Gum disease is one of the most common diseases seen in humans. In its most severe form, known as periodontitis, the gum tissue and bone that support the teeth are destroyed over time, leading to loss of teeth. Periodontitis affects about half of all adults and as many as 85% of people over 65-years of age.
Although diabetes and gum disease may seem like very different diseases, dentists have known for a long time that people with diabetes are more likely to get gum disease. Also, their gum disease may be worse and harder to treat, compared with people who do not have diabetes. If a person’s blood sugar levels are under good control, however, gum treatment is more likely to be successful. But that’s not the end of the story: scientists are now finding that gum disease may also have an effect on diabetes, making blood sugar control more difficult. Is is clear and that keeping the gums healthy is an important part of looking after the overall health of a person with diabetes.
Possible causes of problem pregnancies
Doctors don’t always understand why these sad events happen, but they think that infections and inflammation (part of your body’s response to harm and injury) might be the cause in many cases. Infections could be caused by germs travelling to the womb from somewhere else in the body. One place germs could come from is the mouth.
We all have millions of germs living in our mouths, without doing us any harm. However, when you get gum disease, some of these germs can change and grow in number and cause an infection in your gums. This leads to the breaking down of the tissues and bone that support the teeth – we call this “periodontitis” or severe gum disease. When the gums are infected in this way, some germs can leak into the blood stream when you brush your teeth or bite down hard. If this happens in a pregnant woman, it could be one way for infection to reach the developing baby in the womb. This could then cause health problems for both mother and baby.
What we know about gum disease and problem pregnancies
To find out if having gum disease could really harm a pregnancy or baby, a group of top scientists recently looked closely at the results of all the research done in recent years. They found that there is a link between gum disease and three possible problems: having a baby with a low weight at birth, giving birth too early in the pregnancy, or having dangerously high blood pressure (pre-eclampsia) during pregnancy. This means that having gum disease could slightly increase a woman’s chance of one of these unwelcome pregnancy outcomes.
Scientists think that germs and their products can travel through the blood from the site of gum disease to the womb. In fact, traces of germs from the mother’s mouth have been found in the fluid around the baby and in blood inside the cord that links the baby to its mother. However, a lot more research is needed to prove a “cause and effect” link between gum disease and pregnancy problems. In addition, it is important to understand that there are many things that can affect the health of a woman and her unborn baby – for example, smoking, lifestyle choices and some medical conditions. Having gum disease does not mean that your baby will be harmed, but making sure that your mouth is healthy will give your baby the best chance of a good start.
Care of your gums during pregnancy
If you are planning to become pregnant, or already are, then you should get a check-up from your dentist to see if your gums are healthy. Your dentist can then pick up any early signs of gum disease and the dentist or hygienist can treat any disease you already have. He or she will also give you advice on how to look after your teeth and gums at home. Make sure you go back for regular check-ups, because being pregnant also makes it more likely that you will have gum problems, because of how your hormone levels change during pregnancy.
Keeping your mouth healthy will help you and your unborn child to stay healthy.
Sign up for our newsletter
The EFP publishes a free monthtly email newsletter with the latest news about the federation's activities, its publications, and its campaigns.
EFP partners
Oral Health Partners:

International & European Association Awards
2021 Winner - European Association of the year